
Written by the Progyny Editorial Team. Reviewed by the Progyny Clinical Team — March 2026.
You may think about your menstrual cycle at least once a month, or maybe much more if you’re hoping to become pregnant. But how well do you know what’s really happening in your body? If it’s a little unclear, you’re not alone.
Let’s break down what happens during your cycle and how it relates to pregnancy. If you’re considering fertility treatment, this may also help you understand treatment steps and medicine used.
Your menstrual cycle
We have menstrual cycles to release an egg and prepare the body for pregnancy.
There are 4 phases of the menstrual cycle. We’ll start with a quick overview, then look at each phase in more detail.
- Menstrual phase (period): you shed the lining of your uterus (endometrium).
- Follicular phase: your body gets ready for ovulation.
- Ovulation phase: an egg is released, about halfway through your cycle.
- Luteal phase: the uterus prepares for a possible embryo to implant, or the arrival of your next period.
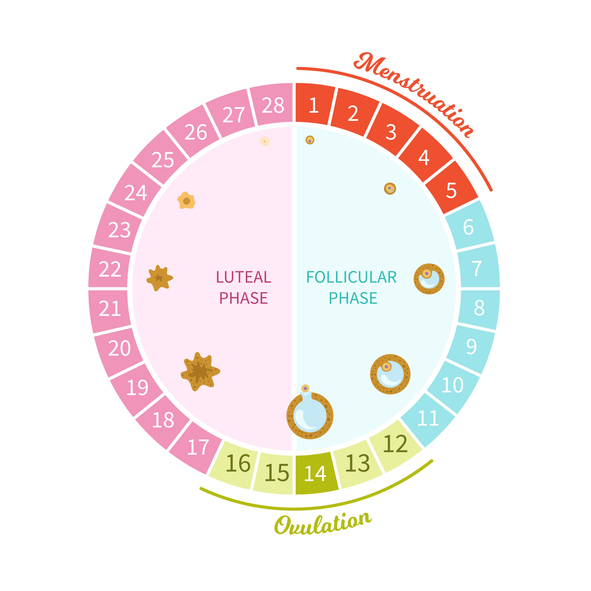
*The number of days in each phase may vary from person to person and even month to month.
1. Menstrual phase
Your cycle begins with the first full day of your period. The bleeding is your body shedding the lining of the uterus (endometrium). Most people bleed for 3 to 7 days.
Hormones in action:
- Progesterone and estrogen drop, causing your period to start
2. Follicular phase
In the follicular phase, your body releases follicle-stimulating hormone (FSH) which causes the ovary to grow follicles. A follicle is a small fluid-filled sac in the ovary that may release and nourish an egg. Only one follicle will be “chosen” to mature.
The growing follicle produces estrogen, which causes the endometrium to thicken. This will make a cozy home for a possible embryo.
Hormones in action:
- FSH rises, causing a follicle to develop
- Estrogen rises, causing the endometrium to thicken
3. Ovulation
When the follicle gets big enough and your body has been exposed to estrogen long enough, there’s a surge of luteinizing hormone (LH). This surge causes ovulation, the release of a mature egg. The egg travels into one of the fallopian tubes.
If an egg meets sperm in the fallopian tube, you may become pregnant. We’ll talk about that timing more in a moment.
Hormones in action:
- LH surges (a sudden rise), causing ovulation
4. Luteal phase
After ovulation, the now-empty follicle (the sac that released the egg) still has an important role. It becomes a temporary structure called a corpus luteum, which is why we call this the luteal phase. The corpus luteum produces the hormone progesterone. Progesterone’s job is to prepare the uterine lining for a possible embryo.
If you become pregnant, your body produces the hormone that’s detected in pregnancy tests: human chorionic gonadotropin (hCG). hCG helps keep the uterine lining thick.
If there is not a pregnancy, progesterone will drop at the end of the cycle. This brings on your period and the cycle begins again.
Hormones in action:
- Progesterone rises, preparing the uterine lining
- If pregnant: hCG rises, keeping the uterine lining thick
- If not pregnant: progesterone drops, starting the cycle again
When should I have sex to get pregnant?
As you know, pregnancy happens when sperm meets the egg. The egg is released at ovulation, around day 14 for most people.
But sperm can live in your body for up to 5 days. So the window to have intercourse begins 5 days before ovulation. Plus, the egg lives for about 1 day, so you have roughly a 6-day window. To learn more about signs of ovulation and how to time intercourse, be sure to read When should I have sex to get pregnant?
Your Progyny Care Advocate is also here to talk through family planning and provide education on topics like this.
Disclaimer: The information provided by Progyny is for educational purposes only and is not medical advice. Always consult a qualified healthcare provider for medical guidance.